This week's broadcast of Mountain Stage is a special episode featuring songs that represent the four seasons of the year. You'll hear live performances by Doc Watson, Bruce Hornsby, Susan Werner, Molly Tuttle, Taj Mahal, Norah Jones and many more.
Home » West Virginians Die Of Diabetes At The Highest Rate In The U.S. A Bill Seeks To Make Treatment More Accessible
Published
West Virginians Die Of Diabetes At The Highest Rate In The U.S. A Bill Seeks To Make Treatment More Accessible
Share this Article
This story was originally published by Mountain State Spotlight. For more stories from Mountain State Spotlight, visit www.mountainstatespotlight.org.
When Maggie Reider’s first-grade son was diagnosed with Type 1 diabetes in 2008, her first thought was “is this a death sentence?”
“My only knowledge [of the disease] was what happened in ‘Steel Magnolias,’” said Reider, referring to the movie that features a diabetic Julia Roberts who dies from kidney failure not long after giving birth to her first child. “I worried things weren’t going to end well.”
Courtesy, Roxy Vasil
/
Roxy Vasil and Maggie Reider.
Then, Reider became more familiar with the disease, which occurs when a person’s body doesn’t produce insulin. It can cause serious organ damage if left untreated, but the Morgantown native learned that with proper management, her son could live a healthy life.
But that management would come with a hefty price tag.
The cost of treating diabetes has made local and national headlines over the past few years, as the price of insulin — used by diabetics to regulate blood sugar — has surged and insurance coverage hasn’t kept up. According to the Health Care Cost Institute, the cost of routine care for a person with Type 1 diabetes was around $18,000 a year in 2016. Prices have gone up since then.
In West Virginia, a state with both the highest diabetes mortality rate in the country and one of the highest percentages of residents living below the poverty line, medicine and equipment required to best treat the disease is inaccessible for many.
Lawmakers are once again considering a bill to lower the expenses for essential diabetic equipment. The bill — introduced with bipartisan support in the House of Delegates — has yet to be assigned to a committee agenda, which is typically the first sign it has a chance of passage.
Technology upgrades
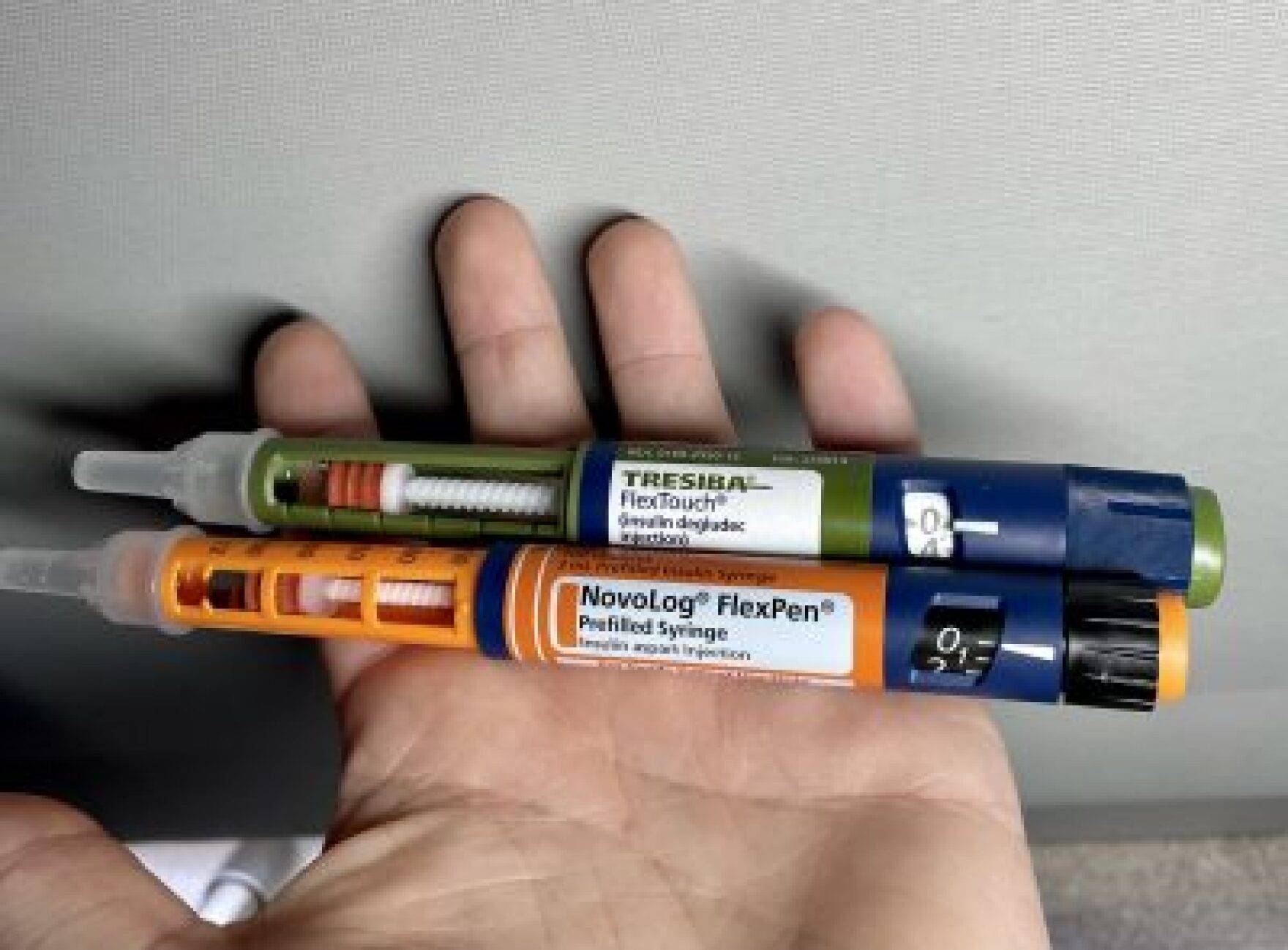
Diabetes management used to just involve finger pricks and test-strips to check blood sugar throughout the day. But as technology has advanced, it’s evolved into sensors, pumps and monitors, which automate the process and provide a more consistent and accurate reading in real time. Studies have shown that these newer methods improve health outcomes, but the equipment is expensive and only available to those who can afford it.
“When we were on simple syringes with insulin vials, it was pricey. But as my son grew older and the technology got better, things became really expensive,” Reider said. “It all adds up. But it’s life-saving, so you make it work.”
For Reider’s family, “making it work” meant picking up a second job.
A widow and single mother when her son was diagnosed, Reider said her schoolteacher salary wasn’t enough to cover the costs of treatment. So, she took a job as a waitress on the side.
When her son, Roxy Vasil, turned 16, he got a job at a funeral home. The money he earned helped pay for sensors for his continuous glucose monitor, which he wears on his arm. It provides continuous monitoring and automatically notifies him when he needs insulin. Before, it was a guessing game — he’d draw blood from his finger periodically throughout the day.
Last year, the West Virginia Legislature passed a bill that capped the copays for insulin at $100 for a 30-day supply in response to the rising cost. Lawmakers who supported the legislation say it was a good first step, but insulin is just one of the many tools needed to manage diabetes.
Now, a house bill with bipartisan sponsorship seeks to go a step further. Sponsored by Del. Matthew Rohrbach, R-Cabell, and co-sponsored by Del. Barbara Fleischauer, D-Monongalia, House Bill 2708 would lower the $100 insulin cap to $25, and in addition to insulin, would apply the same cap to pharmaceutical supplies and equipment, too. rfthy
Courtesy, Roxy Vasil
/
Roxy Vasil uses a Freestyle Libre 14 Day Sensor to monitor monitor his blood sugar levels and keep healthy. It’s one of the technologies that a new house bill wants to make more affordable for diabetic West Virginians.
Rohrbach, a physician who serves as vice chairman of the House Health and Human Resources Committee, did not return requests for comment. But during a panel discussion in early February, Rohrbach said the bill would improve West Virginia’s health, economy and wellbeing.
“We’ve really advanced [in technology used to treat diabetes],” Rohrbach said. “But unfortunately, a lot of people don’t have access because of costs.”
And when preventive treatment is inaccessible, more people get sick and die.
“The long-term consequences of diabetes — the organ damage, the heart attacks, the strokes — we can prevent with better diabetic control,” Rohrbach said.
Those consequences are disproportionately borne by Black West Virginians. According to data from the U.S. Centers for Disease Control, diabetes is the fourth leading cause of death for the state’s Black residents. Nationally, non-Hispanic Black people were twice as likely to die from diabetes as non-Hispanic white people, according to data from 2018.
“What this bill is really an attempt to do is to make it easier for individuals to get access to these lifesaving medications and technologies and limit the effects down the road,” Rohrbach said.
The bill hasn’t been placed on the agenda of the House Health and Human Resources Committee, which means that no testimony for or against the legislation has been heard. But last year, private insurance companies and the state Office of the Insurance Commissioner opposed the bill. They expressed concerns that the capped co-pays would impact the market. The Office of the Insurance Commissioner did not respond to questions about whether there’s been an impact on the market from last year’s legislation.
Fleischauer says similar legislation has already been passed in other states. She said HB 2708 is modeled after legislation passed in Connecticut last year.
“Connecticut has one of the lowest mortality rates for diabetes in the country, and they passed this legislation,” Fleischauer said. “If they can take this step to save lives, we can, too.”
Reider and Vasil both said the legislation would make a huge difference for families like theirs.
“Diabetes doesn’t discriminate. It impacts Democrats and Republicans alike, so I hope lawmakers can come together and pass this for West Virginians,” Reider said.
Vasil, who’s now a freshman in college, said having access to the higher-tech equipment has changed how he’s able to manage the disease.
“I’ve lost weight, my [sugar levels] have improved, and I’m more motivated to keep healthy because of my CGM,” Vasil said. “I think every diabetic should be able to access one.”
The deadline for the bill to pass the House of Delegates — and head to the Senate — is March 31.
Reach reporter Lauren Peace at laurenpeace@mountainstatespotlight.org
Health care services for nearly 30 percent of West Virginia’s population may be difficult to access if lawmakers don’t fully fund the Medicaid program in an expected special session.
On this West Virginia Morning, health care services for nearly 30 percent of West Virginia’s population may be difficult to access if lawmakers don’t fully fund the Medicaid program in an expected special session. Emily Rice has more.
Two deer tested positive for chronic wasting disease in Harpers Ferry National Historical Park, marking the disease's first documented occurrence in the park.