Many West Virginia adults find themselves in the difficult position of caring for their children and looking after their parents at the same time. Conditions like dementia and Alzheimer’s are problems, but so are mobility and safety issues at home. It can be stress-inducing and makes many people wonder if there is any help available and where to get it.
News Director Eric Douglas has found himself in the same position and wondered the same things. Through this interview series, we will bring experts into the studio to talk about things people need to know as they get older, or when helping aging parents.
This week on Inside Appalachia, we visit with West Virginia trappers to learn about the fur trade in the 21st century. We also meet a county fair champion who keeps racking up the blue ribbons and has released a cookbook of some of her favorites. And we hear an update on the Mountain Valley Pipeline. Construction has begun again, but some people wonder if it’s even needed.
This week, we visit with West Virginia trappers to learn about the fur trade in the 21st century.
We also meet a county fair champion who keeps racking up the blue ribbons and has released a cookbook of some of her favorites.
And we hear an update on the Mountain Valley Pipeline. Construction has begun again, but some people wonder if it’s even needed.
These stories and more this week, Inside Appalachia.
Before coal or timber, the fur trade was one of Appalachia’s first industries.
Fur trapping flourished for centuries, made fortunes and led to wars and was still lucrative into the last few generations.
Now, most West Virginia fur trappers struggle to earn a living, but some have adapted or found new careers using their particular skills. Folkways Reporter Lauren Griffin brought us the story.
Blue Ribbon-Winning Fair Food
There’s nothing quite like the county fair, where you can pet a goat or get motion sick on the tilt-a-whirl.
A staple of county and state fairs are the annual craft competitions, where the hopeful vie for the coveted blue ribbon.
Few people have been as successful as Russell County, Virginia resident Linda Skeens, who has won hundreds of ribbons, become a social media sensation and released a cookbook featuring some of her winning recipes.
Producer Bill Lynch spoke with her about winning contests and collecting recipes.
Cruising With Vintage Vehicles
For over 50 years, in Roanoke, Virginia, on any given Friday night, you can see modified cars and trucks with neon lights, spinning rims and streamlined spoilers strutting from north to south and back again. And often — you’ll see old-timey antique cars out there among them.
Host Mason Adams reported this story in 2020, about a family of mechanics who have spent years developing the skills to get those vintage cars just right.
The Mountain Valley Pipeline Saga Continues
We’ve reported on the Mountain Valley Pipeline for years. Completion of the pipeline has been held up because a federal court keeps throwing out its permits. The U.S. Supreme Court recently ruled to allow work to resume again. But some energy analysts question whether the pipeline is even needed.
WVPB’s Curtis Tate spoke with Suzanne Mattei of the Institute for Energy Economics and Financial Analysis.
Extended Family Pitching In To Care For Dementia Patients
Spouses or adult children typically care for people with dementia, but more and more extended family members are taking on that role. CareEx is a project at the Center for Gerontology at Virginia Tech that studies extended family caregivers in central Appalachia.
WVPB’s Eric Douglas spoke with project coordinator Brandy McCann about their work.
——
Our theme music is by Matt Jackfert. Other music this week was provided by the Carolina Chocolate Drops, Sturgill Simpson, Ron Mullennex, Mary Hott and Noam Pikelny.
Bill Lynch is our producer. Zander Aloi is our associate producer. Our executive producer is Eric Douglas. Kelley Libby is our editor. Our audio mixer is Patrick Stephens.
You can send us an email: InsideAppalachia@wvpublic.org.
Millions of families nationwide find themselves caring for loved ones in their own family. Sen. Shelley Moore Capito experienced those issues as she provided care for her own parents. She recently introduced legislation into the U.S. Senate to help alleviate burdens on caregivers.
Millions of families nationwide find themselves caring for loved ones in their own family. That includes stress and confusion — especially when it comes to dealing with a parent’s finances and the services that are available to them.
U.S. Sen. Shelley Moore Capito, R-W.Va., experienced those issues as she provided care for her own parents. She recently introduced legislation into the U.S. Senate to help alleviate burdens on caregivers.
The transcript below has been lightly edited for clarity.
Douglas: We’ve both cared for our parents. Let’s just talk about that experience for a second. So you cared for both of your parents, right? I believe I read that it was your mother first. And then your father began to decline? Or do I have that backwards?
Capito: That’s right. My mother really had a longer slope into full out dementia. She became very isolated, worried about losing her mind. It was sad to watch, but dad could kind of compensate and help her and answer the questions time and time again. And then when he slipped, he went much faster. That was in 2010.
Then it began a long slog for me and my brother and sister to have four years of caring for them, having them being cared for, and trying to figure all this out. It began slow, and then it just all of a sudden, almost one day, we’ve got real issues here.
I think that’s what happens in families, when it’s a couple one can kind of compensate or cover up for the other. And then when that person, when your healthy person goes down, you realize all the things that maybe you should have been paying a little bit more attention to.
Douglas: I asked the question because your father was the caregiver for your mother and did all of those things that we’re discussing. And then when he began to decline, then suddenly it fell to the next generation, to our generation, to step up and to provide that care.
Capito: It was challenging for us in that none of the three of us lived right there. You can always go back and look, and I’m sure you’ve done this yourself, could I have addressed this earlier, sooner or better? But you’re doing the best you can. And I think that’s what caregivers all across this nation are doing.
Douglas: Yeah, I’ve certainly gone in my head. Should have done this? Should have changed this sooner?
I’ll be honest with you, when I see information about newly introduced legislation, I generally don’t pay a whole lot of attention to it. I know how many steps it takes to become finished legislation. But tell me about this bill to alleviate the care or the burden on caregivers.
Capito: I think what I realized from my own personal experience, and then once I became sort of known as somebody who has lived this experience, is that going through all the insurance, every time they were admitted to the hospital, you have to get another document to sign, you signed the same document every time, why can’t the X-rays, or the testing be transmitted from one hospital to the next?
You have the burden of trying to figure out how to care best for your parents, but then all of the hurdles that you have to jump through, whether it’s for insurance purposes, or HIPAA, or the refrigerator breaks down, all of these things just come cascading down. And you end up with a lot of difficulties in terms of trying to figure out procedures, forms, communications, eligibility, whether you’re talking about Medicare or Social Security.
I think we could make it easier on caregivers who are trying to face this, to make it more streamlined, or at least have these agencies look at how they could streamline their processes to make it easier.
Douglas: That was one of the things that I struggled with, who do I go to to find out how to care for my mom? It’s very frustrating.
Capito: You are looking at financial data, too. That’s another thing. I mean, that’s different than what this act for caregivers or alleviating barriers for caregivers would do, but financial institutions, I think could help you a lot more in terms of trying to figure out credit card and bank accounts, so that not only do you have, “How am I going to get the health care? How am I going to pay for this?” And if they can’t communicate to you successfully, where is everything? I don’t know about you, but I spent a lot of time trying to unwind and figure out how to do all this.
It was a labor of love for me, but it was extremely time consuming and emotionally draining. And then you’re trying to have your life at the same time. My parents actually got very, very ill in 2014, which was the year I was running my first Senate race, and I’m like, wow, what am I going to do? Finally my mother, in the memory unit, in September of 2014, when my campaign obviously was almost over in November, my mother died.
I remember a campaign meeting that I had the day before she died. And I just looked at my campaign team, and I said, “I can’t do all this. My mother is dying.” I had no idea she was gonna die the next day, but I could see. And I really think my mother was looking in my eyes going, “She’s really tired. I might as well just hang it up. She needs a break.”
Pictured here with her father, the late-Gov. Arch Moore, in 1962. Shelley Moore Capito was one of her father and mother’s caregivers as they struggled with memory loss later in the life.
Photo courtesy of the West Virginia & Regional History Center/WVU Libraries
Douglas: You were in the U.S. House leading up to that, too. You had a full schedule going on with them and living in D.C., or at least commuting back and forth.
A lot of caregivers, just generally speaking, have moved away, we’ve moved all over the country. Families aren’t located within 10 miles of each other anymore. Who do you call? Who do you rely on?
Capito: I have an older brother and a younger sister. They were very helpful, but at the end of the day, one person ends up making those decisions, and that person was me.
Douglas: Why has the system grown to to be such a challenge for caregivers?
Capito: I think a lot of it has to do with people living longer. It’s not all about dementia, it could be broken hips or heart failure, whatever. I think people are living longer. And so I think that presents a challenge because, are they living healthy all the way to the day they die? Of course not. And so I think that’s a challenge. I think our society is much more mobile, as we said, so many people have moved away from home. We have families that maybe 30, 40 years ago, maybe the wife wasn’t working, but we have many more women in the workforce, dual occupation couples.
My mother’s mother had the same issue in the ’60s and ’70s. Once it was unmanageable at home, she went into a nursing home for like eight years. We don’t do that anymore. And because that’s not the modality that’s really the best treatment for certain types of things. I think that’s got some impact on it. And the cost of caring.
If you can’t quit your job and move across the country, which a lot of people do, it becomes very, very hard and you look at the cost and you say to yourself, it’s probably the least costly way to do it. And the best I’m going to feel about is if I just drop out of the workforce for right now and manage this. So I think it’s all kinds of factors like that.
Douglas: Nationwide, there’s 53 million family caregivers, but even in West Virginia, we’re looking at a quarter of a million people in a state of 1.8 million people. That’s kind of astounding. That’s one-in-eight, one-in-seven people in the state is a family caregiver for another 100,000 people who need the care.
Capito: That’s where something like the Credit for Caregiving Act, which is another one we put out, and it’s been out there for a couple years, to try to give some financial relief in the form of a tax credit for family caregivers. You try to attack it that way a little bit to maybe ease the burden. The nice thing about this issue, which is not too nice, but it’s totally bipartisan, and because this has no barriers in terms of how it hits people in terms of their politics, obviously. It’s one of the issues that we can work on together. I’m a big believer in medical research and development of new therapies and earlier treatment and earlier diagnosis.
So all of these things kind of drive me because of my personal experience, not that I hadn’t seen it in other families but until you hit it yourself, you really don’t understand what’s going on. And so that’s why I’ve sort of taken this on as one of my causes that I think we could make a difference on.
Douglas: Any prognostication on the possibility of this, this moving on through and out of committee and onto the floor?
Capito: This is national Family Caregivers Month, so it’s a good month to be talking about it. The bill probably doesn’t have a burden, but we’ll need to attach it onto another bill going through the Health Committee. We’re looking for those opportunities and it has bipartisan co-sponsorships. We’ve just put it out there. So we’ll see what happens. We’ve been trying to look for what we say is a vehicle to get it passed.
This week on Inside Appalachia, we visit with West Virginia trappers to learn about the fur trade in the 21st Century. We also meet a county fair champion who keeps racking up the blue ribbons and has released a cookbook of some of her favorites. And we hear an update on the Mountain Valley Pipeline. Construction has begun again, but some people wonder if it’s even needed.
This week, we visit with West Virginia trappers to learn about the fur trade in the 21st century.
We also meet a county fair champion who keeps racking up the blue ribbons and has released a cookbook of some of her favorites.
And we hear an update on the Mountain Valley Pipeline. Construction has begun again, but some people wonder if it’s even needed.
These stories and more this week, Inside Appalachia.
Before coal or timber, the fur trade was one of Appalachia’s first industries.
Fur trapping flourished for centuries, made fortunes and led to wars and was still lucrative into the last few generations.
Now, most West Virginia fur trappers struggle to earn a living, but some have adapted or found new careers using their particular skills. Folkways Reporter Lauren Griffin brought us the story.
Blue Ribbon-Winning Fair Food
There’s nothing quite like the county fair, where you can pet a goat or get motion sick on the tilt-a-whirl.
A staple of county and state fairs are the annual craft competitions, where the hopeful vie for the coveted blue ribbon.
Few people have been as successful as Russell County, Virginia resident Linda Skeens, who has won hundreds of ribbons, become a social media sensation and released a cookbook featuring some of her winning recipes.
Producer Bill Lynch spoke with her about winning contests and collecting recipes.
Cruising With Vintage Vehicles
For over 50 years, in Roanoke, Virginia, on any given Friday night, you can see modified cars and trucks with neon lights, spinning rims and streamlined spoilers strutting from north to south and back again. And often — you’ll see old timey antique cars out there among them.
Host Mason Adams reported this story in 2020, about a family of mechanics who have spent years developing the skills to get those vintage cars just right.
The Mountain Valley Pipeline Saga Continues
We’ve reported on the Mountain Valley Pipeline for years. Completion of the pipeline has been held up because a federal court keeps throwing out its permits. The U.S. Supreme Court recently ruled to allow work to resume again. But some energy analysts question whether the pipeline is even needed.
WVPB’s Curtis Tate spoke with Suzanne Mattei of the Institute for Energy Economics and Financial Analysis.
Extended Family Pitching In To Care For Dementia Patients
Spouses or adult children typically care for people with dementia, but more and more extended family members are taking on that role. CareEx is a project at the Center for Gerontology at Virginia Tech that studies extended family caregivers in central Appalachia.
WVPB’s Eric Douglas spoke with project coordinator Brandy McCann about their work.
——
Our theme music is by Matt Jackfert. Other music this week was provided by the Carolina Chocolate Drops, Sturgill Simpson, Ron Mullennex, Mary Hott and Noam Pikelny.
Bill Lynch is our producer. Zander Aloi is our associate producer. Our executive producer is Eric Douglas. Kelley Libby is our editor. Our audio mixer is Patrick Stephens.
You can send us an email: InsideAppalachia@wvpublic.org.
Many families have to move a loved one into a nursing home because of dementia. The experience often comes with grief and loss and a sense of failure.
Many families have to move a loved one into a nursing home because of dementia. The experience often comes with grief and loss and a sense of failure.
For his series Getting Into Their Reality: Caring For Aging Parents, News Director Eric Douglas visited a nursing home in Marmet, West Virginia with a memory care program for people with dementia to discuss the process.
He spoke with Julia Smythe, the dementia program director, and Natalie Petty, the director of admissions and marketing.
The transcript below has been lightly edited for clarity.
Douglas: People only put their family member in a nursing home for the first time once it’s an overwhelming feeling of, “Oh my God, what’s going on? I don’t understand any of this.” There’s a lot of fear. There’s a lot of confusion. And I can speak to that personally. So talk to me about what that’s like. What’s the admission process? What do you do when somebody comes and says, “My mom has dementia. I don’t know how to deal with this, what do I need to do?”
Smythe: What we do is we provide support through resources through the Alzheimer’s Association for caregivers. What I always do is I send out a packet to the family member that includes caregiver stress, how to care for yourself while you’re caring for others, and grieving because during the process of dementia, you don’t grieve once, you grieve several times, because you grieve the loss of each stage.
That’s a very real experience that all family members I talked to experience. So when they’re admitted here, what we do is we have a meeting with the family and we discuss what it’s going to be like living here for their family member. And we include the family members and all activities that they would like, too. They can come in freely and join in on activities and mealtime. You can join in on meals here, too. It’s supposed to be a home-like environment.
When I’m talking with family members about placement, what I usually stress is, it’s the safety of your loved one. That’s what we’re most concerned about. Because when it comes to the placement, most people are at the point where their family member is trying to elope from their home, because they don’t feel safe. They keep saying that they want to go home even though they’re already home. And that’s all because they don’t feel comfortable in their own body.
Our job is to create that comfort through the programming. So that’s really what I talk to family members about to try to ease them. And of course, when they’re here, I encourage them to visit as much as they want unless it causes some behaviors, because it can for some people with dementia, if they think you’re not the person you are. We monitor those things to try to work with family members to see what the best visitation schedule would be for them and how we can use our tools that we do in the beginning.
Petty: When it comes to the financial issues, that is also very overwhelming. So I will also meet with families, tell them where to start, how to start the Medicaid process if needed. We even have some girls in our office that can help walk you through that application and get that submitted. So we help with the steps to that as well.
Douglas: Let’s talk about the admissions process a little bit more.
Petty: Depending on where the family member is, if they’re at home, I usually start with the family. And like we talked about earlier, we bring the family and we talk about what their needs are.
Douglas: Let me back up and ask one question. Do you need a doctor’s referral?
Petty: Yes. That’s usually where I have everybody start, especially if they’re from home, I have them start with their doctor, have them get an appointment with them, let them know what situation they have at home. There is a pre-admission screening form that has to be filled out by the doctor. And we need a little bit of clinical information from that doctor’s visit, we can get that submitted for approval.
And then we start looking at their payer sources, if they have insurance, what type of insurance they have, if they need Medicaid, we start working on that and get everybody started with that process. And then after that, you’re on the referral list. And so it’s just a matter of when we have an open bed. And when all the paperwork gets approved. Once we do that, then we usually contact the family and we set up a time for them to admit their family member.
If it’s from the hospital, a lot of times that works a lot faster than home. It’s a process when they’re at home. But the hospital’s able to bypass your family physician. They have doctors that can fill out that form and they have access to all the clinicals when the patient’s in the hospital so and we have liaisons at the hospital that can come in and assess the patient when need be. So all of that can be fast-tracked through the hospital.
Smythe: I also assess patients in the hospital and at home and other facilities. So I can go into the home as well upon request or they can come and bring their loved one to the memory unit to see how they do interacting with other residents. We’ve done that before, too.
Dementia Experience
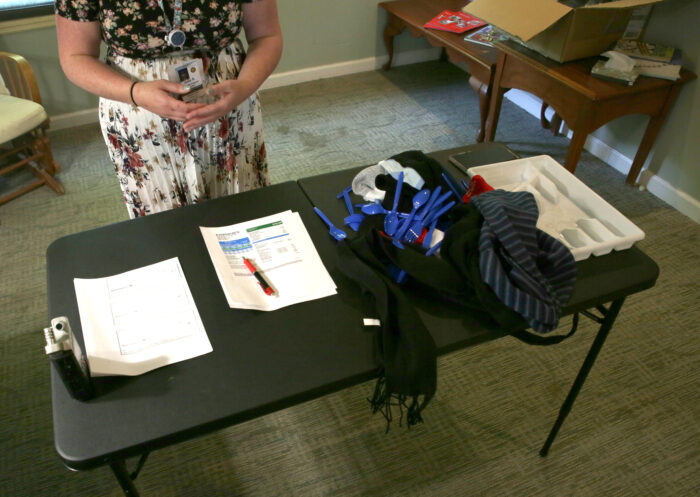
The memory care staff also sets up a community activity to allow family members or members of the community to come in and experience what it’s like to have dementia, including the physical and perceptual challenges.
Julia Smythe explains what will happen in the dementia experience. Credit: Eric Douglas/WVPBItems used in the dementia experience exercise. Credit: Eric Douglas/WVPBItems used in the dementia experience exercise. Credit: Eric Douglas/WVPBhttps://wvpublic.org/wp-content/uploads/2023/06/06XX-Dementia-experience-1.mp3
Listen above to Julia Smythe explain the dementia experience in this bonus audio content.
The transcript below is from the dementia experience.
Douglas: Tell me what you’re doing here today.
Smythe: We are running a dementia experience. We dull your senses to the point that someone with dementia would be feeling. We want you to try and to take on everyday tasks with your senses dulled to see how difficult it is to do your activities of daily living. What we do is we put gloves on you, we put little earplugs in your ears, we put a hat over your head, we put prescription glasses on, and then sunglasses over those. The reason for that is when somebody has dementia or Alzheimer’s, their vision is greatly affected. They usually have tunnel vision, their peripheral is very dark. That’s what causes a lot of falls and mobility issues. We also put rice in your shoes. And so the rice in the shoes is to show you how off balance somebody is when they are not able to feel their extremities the way they used to. You can see the shuffled gait or the high risk of falls with the rice in the shoes.
What we do is we have you put all of those things on, and then you have to attempt to get dressed and put a piece of jewelry on. And then we move to the second station. That’s our office station where we have you read these bills here. And then we will have you fill out these checks. And we want to see if you can match the amount with the correct amount on the form here. Running this experience, we’ve seen that with all of the gear on, it’s extremely difficult to find these lines. It’s extremely difficult to write the same way that you normally would. Your handwriting is not as legible.
That’s actually one of the things that I noticed about my grandmother when she first started getting sick. She used to write scripture all day, and I noticed that her handwriting was getting worse. And then that’s when all of the cognitive issues started and she started being looked at for dementia.
It’s little things like that when you notice trouble with finances and then the inability to write or verbalize things the way that you used to.
Then we have our assorted folding station. As you can see, it’s a jumbled mess. You have to attempt to fold the scarves that we have here. And then you have to match all of the socks. And then you take all of the utensils here, and you have to separate them into our utensil bin here. So this is a very difficult station here because you can’t feel your fingers too well. And it feels like you have really big hands.
Our last station over here is pill sorting. Because of the gloves you can’t feel where the pills are.
Members of the community interested in going through the dementia experience can call the Genesis Marmet Center to schedule an appointment.
A real problem facing many older adults is having enough money for their retirement. News Director Eric Douglas spoke with Josh Hodges, the chief customer officer for the National Council on Aging, to learn about the help that is available for retirees and caregivers.
A real problem facing many older adults is having enough money for their retirement.
News Director Eric Douglas spoke with Josh Hodges, the chief customer officer for the National Council on Aging (NCOA), to learn about the help that is available for retirees and caregivers.
This interview has been lightly edited for clarity.
Douglas: Do me a favor, start out by giving me a quick introduction of who you are and what you do.
Hodges: Josh Hodges, I’m the chief customer officer at the National Council on Aging, or NCOA. We’re a national nonprofit, have been around for about 75 years, focusing on helping people age well. That can mean a bunch of different things. We have programs on the health aspects, focusing on helping people live healthy, planning for that stage of their life. We have employment opportunities.
We also have a lot of opportunities around economic security to help people have the money they need in retirement, help them stretch their dollars. I’ve been at NCOA for about four and a half, almost five years. Before that I spent over 10 years with the federal government doing aging programs.
Douglas: What are some of the tips that people need to know, as they’re getting older, as they’re getting into retirement age, to care for themselves and plan for the future?
Hodges: Well, they are two major drivers of running out of money. First, longevity. People live longer than they expect. For a 65-year-old, there’s a decent chance you’re gonna live to be 85. That’s especially true for women. There’s also long-term care costs of longevity, and then the cost of care later in life.
As any caregiver knows, long-term care is a series of caregiving opportunities that you need to help older adults continue to live in a home, or in an assisted living facility type place. And long-term care can be extremely expensive. It’s one of the things people don’t like to talk about, we don’t like to talk about the fact that we may need help getting around our community, we need help getting around the house, or making meals. We don’t, as a society, like to talk about those things.
Long-term care is really driving the fact many older adults age into poverty, again, especially true for women. So, one thing we like to do in NCOA is really focus on — how do we help you stretch your dollars? There are federal programs out there and state programs out there to help you really make your money work every month. These are programs that you can apply for that have certain qualifications about their age, or income qualifications, that really help people make those daily expenses possible.
Douglas: Let’s talk about some of those programs, some of the ways that seniors can stretch their dollars to survive 20 or 30 years without a direct income stream other than retirements and social security.
Hodges: I would use some of these programs as supplements, opportunities to help you make those dollars do more. For example, Medicare is not free. Many people think it’s free, it’s this free program at the end of their life where they have access. There are premiums, there are co-pays, there are drug costs to it, and each of those areas have programs to help low-income older adults pay for those things.
One program to help pay for prescription drugs can save somebody an average of $5,000 a year. Now imagine you’re an older adult living in poverty, living at, you know, $12, $14, $15, $20,000 a year — $5,000 in your pocket is pretty significant and it gives you access to the drugs. What we don’t want is what happens in this society, is that people trade off their medication for their food, for their housing, they’re making these incredibly challenging tradeoffs. Having the opportunity to actually connect to these programs to help pay for food, pay for housing, pay for electricity, pay for your Medicare, are our opportunities that we really want to make sure older adults understand.
Douglas: What’s the scale? I mean, when you see TV advertising, you see happy senior citizens out traveling the world and going on vacations. I think we all know in the back of our heads that, that’s not reality for most people. But do you have any sense of the scale of how many people are just kind of eking by versus the ones who are living their best retirement?
Hodges: Our data shows tens of millions of older adults are barely making ends meet. You’re describing the idealized retirement. You get your gold watch after 40 years in a corporate job, then you move off to the Bahamas and you have a nice drink with an umbrella. That’s not the reality for many, many people in this country, because there are just so many different costs at play here. And because again, people are underestimating how long they’re going to live and definitely underestimate how much things cost.
These programs I’m talking about, there are $30 billion, that’s billion with a B, left on the table every year. These are dollars that older adults do qualify for but aren’t actually applying and getting benefits because many of them don’t even apply.
Douglas: In trying to care for my mom, that was one of the issues that I kept running into as a caregiver, I didn’t have a clue how to even get started with that kind of stuff. Where does somebody go to learn about these programs and get signed up for or get registered to take advantage of them?
Hodges: I think you really identified the first major hurdle, just knowledge of these programs. So NCOA runs a website — benefitscheckup.org. It helps people understand what benefits they may qualify for. We’re a nonprofit, we’re not trying to sell you anything. We’re not trying to collect your information, we’re not going to even ask you for your email address. We’re just going to ask you some basic demographic information about yourself, what zip code you live in, how many people live in your household, whether you’re a veteran or not. Some of these programs are dependent on veteran status.
This website gives you a sense of what coverage you may qualify for, then we connect you to where you actually apply for the benefits, because so many of these benefit programs are actually on state websites, are on third party websites. We want to connect you right to the programs themselves.
Douglas: What are the numbers we’re talking about? What does the average older adult qualify for?
Hodges: Average is a hard thing to do. We see many older adults who qualify for a Medicare savings plan or extra health. These are programs, they’ll pay for your Medicare. Extra Help is a program to help pay for your prescription drugs, we see numbers above $5,000 a year. Now it depends on what prescription drugs you’re on, it depends on your individual situation. But we’re not talking about pennies here, we’re talking about hundreds if not thousands of dollars.
The bottom line for an older adult or a caregiver: take a look. If you don’t qualify, you don’t qualify, but there are many programs out there designed to help older adults. Some of them are not income dependent. There are programs to help in different parts of the country, too, for local transportation that’s age specific, but not income specific; programs like the National Parks Pass to let you get into the national parks. Many people don’t know these things exist, but they’re out there to save you money.
Douglas: What haven’t we talked about?
Hodges: I think there are really two things to stop people from applying for these benefits. The first is knowledge, and so that’s one of our goals, get information out there. The second is this thought that there are people out there who need the benefits more, so I shouldn’t apply, because I’m doing okay. But these programs expand to meet the eligible individuals. If you don’t apply for the benefit that you would qualify for, somebody else doesn’t get more money. So don’t let that stop you, don’t prevent you from applying for these benefits. These benefits are there for people at all sorts of different income levels. And again, it takes about five minutes to see if you’re qualified for them.
If you prefer a one-on-one approach, we run a national call center. And you can give them a call between 8 a.m. and 8 p.m. eastern, seven days a week to talk to folks. That number is 1-800-794-6559. You can call them, and they’ll actually walk you through what benefits you might be eligible for or connect you to a local resource.
A new study has found that older adults with chronic health issues like heart disease and chronic obstructive pulmonary disorder are much more likely to also have problems with memory loss.
The researchers analyzed three years of data from an annual Centers for Disease Control and Prevention-assisted phone survey. All 50 states, the District of Columbia and several U.S. territories participated.
They found that more than 1 in 10 adults over the age of 45 reported they experienced worsening memory loss within the past 12 months. And that those who experienced cognitive decline were also significantly more likely to have at least one chronic condition.
Those with a history of stroke, chronic obstructive pulmonary disease and heart disease were three times more likely to also self-report cognitive decline. The research suggests patients and providers should be aware of the increased risk of cognitive decline with the presence of chronic diseases — especially since memory problems can complicate care.
The study was published this month in the journal Innovation in Aging and was funded by the Centers for Disease Control and Prevention.
Appalachia Health News is a project of West Virginia Public Broadcasting, with support from Marshall Health and Charleston Area Medical Center.